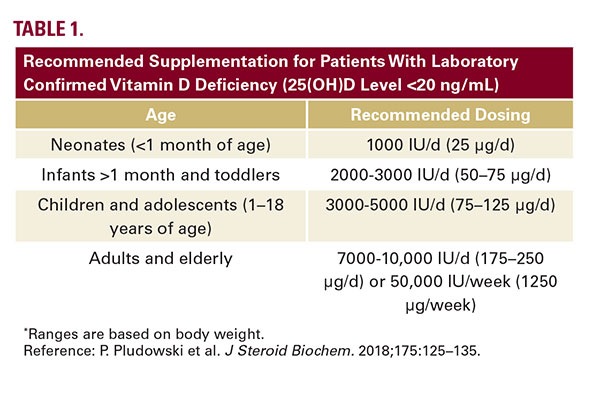
and 800 IU/d (20ug) for adults aged over 70 years to maintain a 25(OH)D concentration of 20ng/mL or higher. However, in individuals who are deficient in Vitamin D (25(OH)D level <20 ng/ mL), of which patients with skin of color are at a higher risk, supplementation is considerably higher. These recommendations are summarized summarized in Table 1.5
Numerous studies have addressed the relationship between Vitamin D and respiratory tract infections. A recent meta-analysis incorporating data from 21,000 patients showed that subjects with Vitamin D levels less than 20 ng/mL had a 64% increased risk of community-acquired pneumonia.6 An additional meta analysis of data from 10,933 subjects from 25 randomized controlled trials documented an overall protective effect of Vitamin D supplementation against acute respiratory tract infection. Protective effects were observed in those receiving daily or weekly dosing of Vitamin D and were strongest in patients with baseline levels less than 25nmol/L than in those with baseline levels greater than 25nmol/L.7
Recent investigations suggest a potential relationship between Vitamin D levels and COVID-19 mortality rates. Laird et al conducted a literature search of Vitamin D status in European countries, which were selected based on the severity of COVID-19 infection. Low Vitamin D concentrations were associated with increased mortality. Countries with a formal Vitamin D fortification policy appeared to have the lowest rates of infection while countries with no policy and highest deficiency rates appeared to be more adversely affected.8
Daneshkhah et al analyzed data from hospitals and clinics in Europe, Asia, and the United States. They noted that patients from countries with high COVID mortality rates had lower vitamin D levels compared to countries that were not as severely affected. There was a strong correlation between Vitamin D deficiency and cytokine storm characterized by a hyperinflammatory, overactive immune response common in patients with COVID-19.9
CONCLUSIONS
Vitamin D deficiency has been well documented in people
of color, in particular AA. The aforementioned
data
suggest a relationship between low Vitamin D status and
COVID-19 mortality rates. While myriad socioeconomic and
health care disparities may be contributing factors, we must
indeed consider key biological variables, including
Vitamin D
status, that may impact these observations. Future prospective
studies are necessary to confirm these findings. As there is currently
no readily available treatment or vaccine for COVID-19,
treating physicians should be cognizant of the higher prevalence
of Vitamin D deficiency in skin of color populations and its
emerging potential role in COVID-19 outcomes. Given the devastating
statistics of COVID-19 among minority communities and
the multifaceted role of Vitamin D in skin and systemic health,
dermatologists are essential partners in decreasing health care
disparities by initiating the vitamin D dialogue. As such, we can
play an invaluable role in improving the health outcomes of our
patients, particularly people of color, during and beyond the
COVID-19 pandemic.
DISCLOSURES
The authors have no relevant conflicts to report.
REFERENCES
1. Centers for Disease Control and Prevention. COVID-19 in Racial and Ethnic Minority Groups. 2020. Available from: URL: https://www.cdc.gov/ coronavirus/2019-ncov/need-extra-precautions/racial-ethnic-minorities.html. Accessed May 12, 2020
2. Ginde AA, Liu MC, Camargo CA Jr. Demographic differences and trends of Vitamin D insufficiency in the US population, 1988-2004. Arch Intern Med. 2009;169(6):626-32
3. Taksler, G., Cutler, D., Giovannucci, E., & Keating, N. Vitamin D deficiency in minority populations. Public Health Nutr. 2015;18(3):379-391.
4. Yang CY, Leung PS, Adamopoulos IE, Gershwin ME. The implication of Vitamin D and autoimmunity: a comprehensive review. Clin Rev Allergy Immunol. 2013; 45(2):217-26.
5. Pludowski P, Holick MF, Grant WB, et al. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol. 2018;175:125-135. doi:10.1016/j.jsbmb. 2017.01.021
6. Zhou YF, Luo BA, Qin LL. The association between Vitamin D deficiency and community-acquired pneumonia: A meta-analysis of observational studies. Medicine (Baltimore). 2019; 98(38):e17252.
7. Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583. Published 2017 Feb 15. doi:10.1136/bmj.i6583.
8. Laird E., Rhodes J., Kenny R.A. Vitamin D and inflammation: potential implications for severity of Covid-19. Ir Med J. 2020;113:81
9. Daneshkhah A., Agrawal V., Esheim A. 2020. The possible role of Vitamin D in suppressing cytokine storm and associated mortality in COVID-19 patients. MedRxiv. https://doi.org/10.1101/2020.04.08.20058578
2. Ginde AA, Liu MC, Camargo CA Jr. Demographic differences and trends of Vitamin D insufficiency in the US population, 1988-2004. Arch Intern Med. 2009;169(6):626-32
3. Taksler, G., Cutler, D., Giovannucci, E., & Keating, N. Vitamin D deficiency in minority populations. Public Health Nutr. 2015;18(3):379-391.
4. Yang CY, Leung PS, Adamopoulos IE, Gershwin ME. The implication of Vitamin D and autoimmunity: a comprehensive review. Clin Rev Allergy Immunol. 2013; 45(2):217-26.
5. Pludowski P, Holick MF, Grant WB, et al. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol. 2018;175:125-135. doi:10.1016/j.jsbmb. 2017.01.021
6. Zhou YF, Luo BA, Qin LL. The association between Vitamin D deficiency and community-acquired pneumonia: A meta-analysis of observational studies. Medicine (Baltimore). 2019; 98(38):e17252.
7. Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583. Published 2017 Feb 15. doi:10.1136/bmj.i6583.
8. Laird E., Rhodes J., Kenny R.A. Vitamin D and inflammation: potential implications for severity of Covid-19. Ir Med J. 2020;113:81
9. Daneshkhah A., Agrawal V., Esheim A. 2020. The possible role of Vitamin D in suppressing cytokine storm and associated mortality in COVID-19 patients. MedRxiv. https://doi.org/10.1101/2020.04.08.20058578
AUTHOR CORRESPONDENCE
Pearl E. Grimes MD [email protected]

